Air quality surveillance and control: How to improve the response to all respiratory diseases, COVID-19 included
By Laura H. Kahn | September 8, 2021

The United States could have been ready for the COVID-19 pandemic. Had federal, state, and local governments devoted significant resources to fighting influenza (aka flu) through vaccination and improved air quality and infection control standards in buildings, the country would have been prepared for other respiratory diseases. The failure to institute these common-sense responses has not only led to unnecessary flu deaths in preceding decades but deepened the COVID-19 crisis.
In May 2016, I wrote a Bulletin piece describing how the United States’ abysmal vaccination rates against seasonal flu predicted a poor performance against future pandemics. Sadly, this prediction has proven true. The US response to the COVID-19 pandemic has been abysmal.
In general, the United States has a poor track record in terms of preventing respiratory pathogens (i.e. deadly microbes) such as flu from spreading, relying on flu vaccines with low efficacy rates to reduce people’s susceptibilities. Vaccine hesitancy, a focus on food-borne and water-borne rather than respiratory pathogens, and poor indoor air quality, circulation, and filtration combined to set the United States up for failure in its COVID-19 response and leave the country vulnerable to other emerging respiratory diseases.
The long history of vaccine hesitancy. Vaccine hesitancy is nothing new. Opposition to vaccination has existed since Edward Jenner scratched cowpox pus into 8-year-old James Phipps, rendering him immune to smallpox. But the public came to accept vaccines as they were shown to be effective against the now largely forgotten terror that scourges such as polio inflicted each year. Since 1979, there have been no domestic cases of polio in the United States. But over time, vaccines have become a victim of their own success. Unscientific and illogical as their beliefs may be, significant numbers of people fear safe and effective vaccines, rather than the diseases they can prevent or limit.
Since the flu virus changes from year to year, influenza vaccine efficacy rates never exceeded 60 percent; experts have had to guess which viral strains were most likely going to circulate in the subsequent year. Egg-based technologies that hadn’t changed in decades were used to manufacture the vaccines before the next flu season.
People don’t fear the flu. Vaccine hesitancy contributes to fluctuating vaccination rates that differ tremendously between states. In adults over 18 years of age, the rates have never reached the national target of 70 percent. Instead, they hover around 50 percent.
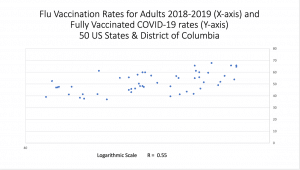
I compared the fully vaccinated COVID-19 rates in American states with flu vaccination rates of 2018-2019 (the year before COVID-19 hit) to see if there was a correlation. (Note: New Jersey and the District of Columbia’s rates were inexplicably absent from 2018-2019, so I used the rates from 2019-2020).
There was.
Many states with low flu vaccination rates also had low COVID-19 vaccination rates. Wyoming and Mississippi had among the lowest rates, while Rhode Island and Massachusetts had some of the highest. The correlation was moderately strong.
Each year, the United States accepts millions of cases, hundreds of thousands of hospitalizations, and tens of thousands of deaths from the flu—even though simple measures to limit the spread of that disease could greatly reduce the toll.
Revelations from COVID-19. Widespread social distancing and face mask wearing during the COVID-19 pandemic produced a salutary side effect: historically low levels of flu and other respiratory diseases. Emergency room visits for pediatric asthma attacks plummeted. And, astonishingly, lockdowns for COVID-19 led to a reduction in premature births.
These phenomena suggest that the respiratory pathogens have a much greater impact on general health than previously realized.
Unfortunately, public health officials have a poor understanding of how respiratory pathogens such as influenza and coronaviruses spread in indoor settings. In making their recommendations on responses to respiratory disease, they use arbitrary divisions such as five microns for respiratory particle sizes and vague definitions such as droplets, droplet nuclei, and aerosols. The result can be baffling and inconsistent public messaging.
But it’s not their fault.
The information that health officials use to base their recommendations on respiratory disease prevention is outdated because there has been scant research on airborne disease transmission in recent years. The research is challenging to do and hasn’t had the support needed to improve it.
The United States (and many other countries) have set up surveillance systems to monitor food-borne and water-borne illnesses. But the United States has not instituted surveillance systems to monitor indoor airborne illnesses. Collecting food and water samples to test is easy. Collecting air samples (particularly indoors) is not. Surveillance of influenza relies on laboratory clinical testing of samples from people exhibiting flu symptoms—not on indoor air surveillance.
This gap in airborne disease surveillance has resulted in a data vacuum for COVID-19. A long lag time occurred before health officials recommended that the public wear face masks. Over a year after the SARS-CoV-2 virus emerged from Wuhan, China, health officials still argued whether COVID-19 was airborne spread or not. There’s scant data on how the Delta variant spreads and, therefore, confusing guidance on how schools and businesses can open safely in the face of the Delta variant.
In general, US society ignores infection risks from indoor air. The design and construction of buildings and other structures (e.g. aircraft, ships) for the most part do not include modifications that could reduce airborne disease risks. And the COVID-19 pandemic has shown the importance of reducing indoor airborne disease risk.
Given what is known now about the importance of indoor air quality and the need to reduce the spread of indoor airborne pathogens, support for respiratory pathogen transmission research needs to be increased, and governments need to adopt building codes and regulations that ensure indoor air quality. Governments at all levels also should foster better ventilation and filtration that reduces airborne disease spread improved surveillance of indoor air pathogens.
For example, improved heating, ventilation, and air conditioning systems, air cleaners, and filtration using high efficiency particulate air (HEPA) filters would improve air quality and reduce respiratory disease spread in school classrooms, offices, restaurants, theaters, and other venues. Modern airliners circulate fresh air and recycle air using HEPA filters, so coronavirus spread on planes is low, but air quality on subways can be highly polluted. Air-quality monitoring should be done regularly along with improvements in ventilation and filtration systems.
Let’s not let the lessons of this pandemic go to waste. It’s time to improve national and world capabilities to prevent the spread of all respiratory pathogens. To accomplish that, governments around the world need to support better surveillance, improved vaccines, reduced vaccine hesitancy, and safer indoor air.
Together, we make the world safer.
The Bulletin elevates expert voices above the noise. But as an independent nonprofit organization, our operations depend on the support of readers like you. Help us continue to deliver quality journalism that holds leaders accountable. Your support of our work at any level is important. In return, we promise our coverage will be understandable, influential, vigilant, solution-oriented, and fair-minded. Together we can make a difference.
Get alerts about this thread
0 Comments
Oldest

Laura H. Kahn
Laura H. Kahn is a physician and policy researcher and is the author of Who's in Charge? Leadership during Epidemics, Bioterror Attacks, and Other Public Health Crises. ... Read More













