Mpox is down but not out: Why a waning outbreak is no cause for complacency
By Matt Field, Dimie Ogoina | April 17, 2023
 An illustration of the mpox virus. Credit: Stephanie Rossow via CDC Public Health Image Library.
An illustration of the mpox virus. Credit: Stephanie Rossow via CDC Public Health Image Library.
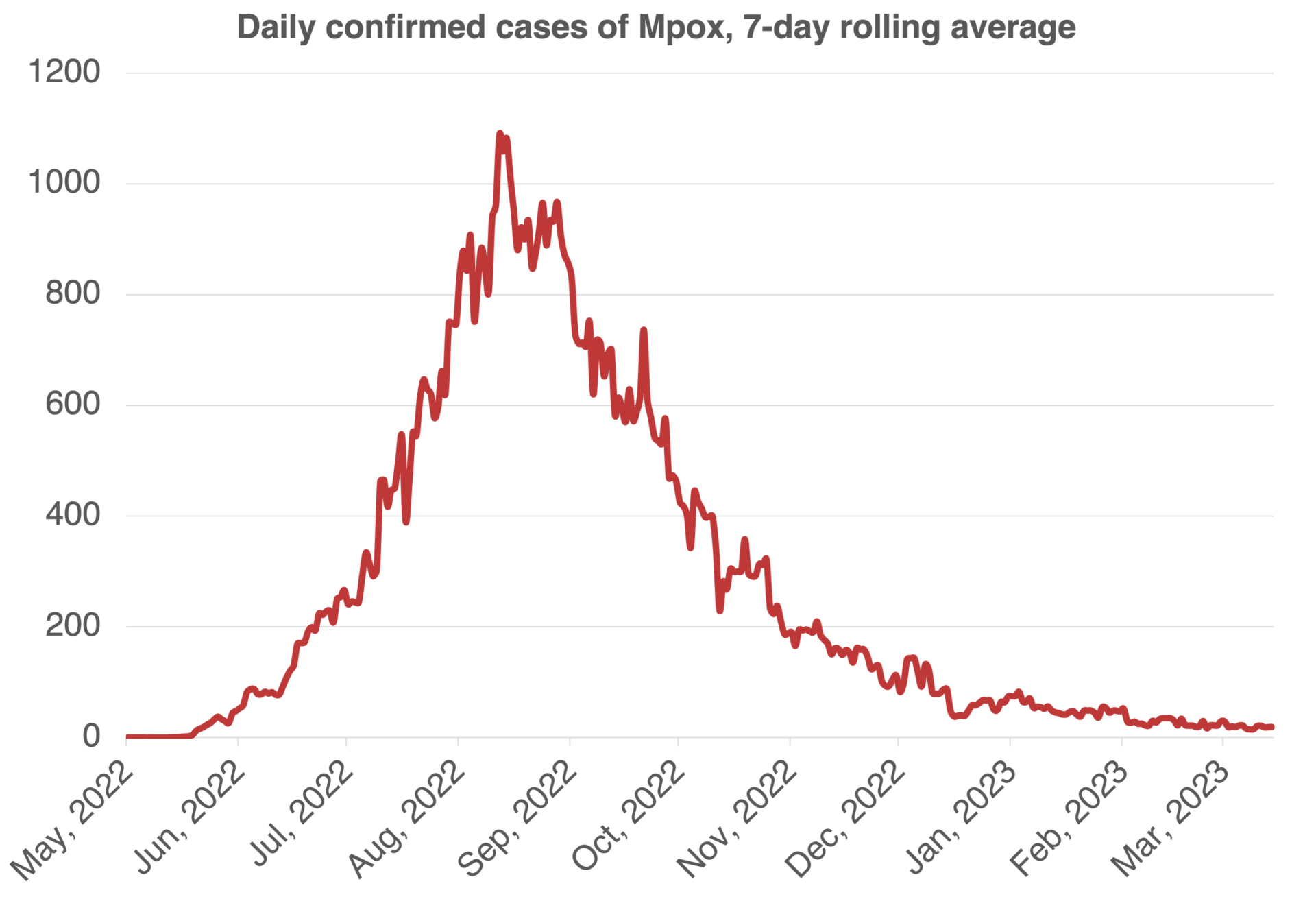
Just a few months ago, mpox looked like it was gaining a toehold outside of a handful of African countries where the disease is considered endemic. In countries like the United States, there were fears that the virus could start percolating in child care centers and other settings, becoming impossible to vanquish. But as countries rolled out effective vaccines, mpox cases began to drop. Over the spring and summer, the United States was reporting hundreds of cases each day, but in March, the seven-day average never topped three. Many other countries have seen the same trend.
Since the global outbreak of mpox (formerly known as monkeypox) began in 2022, 10 countries in Africa have reported 1,463 confirmed cases, a number that is still likely a large undercount. In addition to a lack of the vaccines and therapies that have flooded countries like the United States, some nations in Africa lack the diagnostic capacity to tally up the virus’s true toll. While the unprecedented international wave of infections that began last year has receded, a response that meets continuing infections in Africa with too few resources means the threat of mpox hasn’t. The history of this virus reveals a pathogen that has continuously evolved, shifting how it transmits and whom it affects. At times, during this history, public health authorities have failed to pay adequate attention to mpox.
Doing so again would be a mistake.
Global spread. The current mpox outbreak has proven atypical. In the past, many cases could be tied to animal-to-human transmission, but in the outbreak that began in May 2022, almost all cases have been due to person-to-person transmissions. The first four cases were confirmed in the United Kingdom without an epidemiological link to endemic countries in Africa. Since then, more than 86,000 cases in 110 countries have been reported.
In contrast to the past, when zoonotic transmission and transmission among close household contacts played a major role in spreading mpox, this time, over 84 percent of cases with available data on sexual orientation have been have been among men who have sex with men. The outbreak has been “overwhelmingly concentrated” within networks of these men, the World Health Organization (WHO) has said, raising suspicions that the first-ever community transmission of the virus outside Africa was fueled by sexual activity.
Even as the virus has shifted its geographical range, the current cases likely have their roots in an outbreak nearly six years ago, one that one of us (Dimie Ogoina), along with his colleagues, had a hand in identifying in 2017.
Genomic analysis has revealed that the current outbreak likely stems from a case or cases from an endemic country, “potentially representing the continuous circulation and evolution of the virus that caused the 2017–2018 Nigeria outbreak.” Then, the first case was an 11-year-old boy with a skin rash and mouth sores. To confirm suspicions that what Ogoina and his team was seeing was what is now called the Clade IIb strain of mpox, they had to send the boy’s samples abroad, to Senegal and the United States.
Where mpox had previously been largely confined to rural areas, the 2017 outbreak was the first time in history that the disease was clustering among young adults who lived in urban settings and among those who had no prior contact with wildlife. With the 11-year-old patient, who had no established source of infection, the Clade II mpox had re-emerged in Nigeria after a 38-year hiatus. By the end of 2018, 122 cases were laboratory-confirmed. Many of the cases were in adult men—78 percent of patients were between 21 and 45 years and 69 percent were men. In most of the mpox cases—60 percent—there was no known source of infection. This was the largest outbreak of the Clade IIb strain. Before it began, only 11 mpox cases had ever been reported in West Africa.
Other novel findings from the 2017 outbreak that might seem familiar to anyone following the current outbreak include the incidence of more severe disease in those with advanced HIV disease. The observation of high rates of genital ulcers among some young men who reported multiple sexual partners also led clinicians to suspect transmission of mpox via sexual contact, foreshadowing the current outbreak.
Beginning in 2018, international travelers exported mpox cases from Nigeria to Europe and the United States. Although these cases didn’t spark massive outbreaks, they were early signs of the potential of the virus’s ability to spread globally.
The roots of mpox. In its first decade, mpox cases were restricted to lab animals. In 1958, the Dutch virologist Preben von Magnus and his colleagues isolated the new orthopoxvirus from captive monkeys that had developed a pox-like illness after being imported to Denmark from Singapore. This led to the flawed name “monkeypox” that stuck for decades. The virus belongs to the same genus as the variola virus (the cause of smallpox) and has, in animals, a clinical presentation closely resembling human smallpox. Between 1958 and 1968, eight other outbreaks were reported in non-human primates, the majority in animals exported from Asia to Europe and the United States. However, surveys for orthopoxvirus antibodies suggested the virus might have origins in Africa.
During the decade of animal outbreaks, no human cases were reported, even among people in close contact with affected animals. Due to improvements in animal shipping and the adoption of in-country animal breeding by laboratories in the United States and Europe, the animal outbreaks of mpox ceased after 1968.
The first shift. A major new chapter in the story of mpox occurred in August 1970. That’s when the first-ever human case was confirmed in a 9-month-old boy living in a small village in the Democratic Republic of the Congo (DRC). While the source of his infection could not be identified, researchers suspected that zoonotic transmission could be responsible. The area had a large population of monkeys and apes, and for the boy’s family, like many others in the surrounding population, the primates were part of the local diet. However, no other human infections were detected in the boy’s village.
Between 1970 and 1979, 47 human mpox cases were later confirmed in five African countries, including the DRC, Liberia, Sierra Leone, Nigeria, and Cote d’Ivoire. Of the 47 cases, 38 were reported from the DRC. The cases were mostly in young children, and nearly all were attributed to animal-to-human spillover events in the tropical rainforest areas near the small villages where each of the cases lived.
Mpox’s cousin, smallpox, had long been one of humanity’s great scourges. Following the success of a global effort to eradicate smallpox in 1980, the World Health Organization (WHO) began intensive population surveillance from 1981 to 1986 to ascertain if mpox had replaced smallpox as a threat to human health. This led to the detection of 404 mpox cases in seven African countries, including 386 cases from DRC.
Zoonotic transmission was suspected in most of the cases, which were mainly among younger children, while limited household-related person-to-person transmission was also reported. For primary cases, men and women were equally affected, but there were slightly more women among the secondary cases, likely a result of mothers caring for their sick children. Most cases of mpox typically presented with an early fever accompanied by pox-like skin eruptions, often starting on the face and then spreading to other parts of the body. This usually cleared up within two-to-four weeks. The majority of cases the WHO found during this period were of mild disease, but deaths were highest among smallpox-unvaccinated children.
In March 1986, the WHO committee on orthopoxviruses reviewed the human mpox epidemiology and concluded that the virus was a rare zoonosis in which human-to-human infection sometimes occurred; observed that the disease was not a serious public health problem; and recommended that WHO involvement in mpox surveillance and research should be phased out.
Arguably, turning attention away from mpox was a grave mistake. As we now know, the virus had several more tricks up its sleeves.
A second shift. Between August 1996 and August 1997, an unusually large outbreak of human mpox was reported in three regions in the DRC, including Katako-Kombe, Sankuru sub-region, and Kasai Oriental. These outbreaks were caused by the Congo Basin Clade (now renamed Clade I) of the virus. A total of 419 possible and probable cases were reported and remarkably, this time, a majority, 78 percent, were secondary cases resulting from human-to-human transmissions. The majority of the cases had mild clinical disease and prior smallpox vaccination was protective against disease. The outbreak occurred during a period of civil unrest and economic collapse in the region. One hypothesis is that as people fled to forests in search of food, they came into increased contact with the virus.
Beginning in 2001, the annual mpox case burden progressively increased in the DRC from about 400 to over 3,000 cases in 2013, with associated chains of human-to-human transmission, including a hospital outbreak. During this time, changes in the Clade 1 genome might have increased the virus’s adaption to the humans.
Mpox on the move. In 2003, the mpox virus once again hitched a ride outside of the African countries where it is endemic, this time sparking an outbreak in humans in the United States. The virus travelled not in lab monkeys as it did in the 1950s but in pet prairie dogs and rodents imported from Ghana. The outbreak, caused by the Clade IIa strain (West African Clade), underlined the public health threat mpox could pose to countries outside Africa. Researchers found that people around commercial rodent-trapping sites in Ghana had antibodies to orthopox viruses, potentially indicating that subclinical infections were going unrecognized by health systems. The appearance of mpox in the Western hemisphere bolstered research into the disease and new laws were passed regulating animal trade. It was during the US outbreak that it was clearly shown that the disease due to Clade 1 (Congo Basin Clade) was more virulent than Clade IIa and IIb (the strain responsible for both the 2017 Nigerian outbreak and the global outbreak that began last year 2022) and that the route and type of exposure to the virus could influence the clinical course of human mpox.
Almost all aspects of the epidemiology of mpox have changed since the discovery of the virus in 1958. Possibly, the most remarkable changes started before or during the 2017 Nigeria outbreak, when the virus showed signs of being sexually transmissible and of being adversely associated with advanced HIV. The global spread of a neglected disease has once again shown that infectious pathogens have no borders. Although the incidence of mpox continues to decline globally, there are still many unknowns about the disease, especially in Africa, where the disease remains endemic. Unless deliberate investments are made to better understand the disease and enable equitable access to mpox-related vaccines and therapeutics for mpox prevention and control, the virus is likely to change further and re-emerge in future again as a public threat to all countries.
Together, we make the world safer.
The Bulletin elevates expert voices above the noise. But as an independent nonprofit organization, our operations depend on the support of readers like you. Help us continue to deliver quality journalism that holds leaders accountable. Your support of our work at any level is important. In return, we promise our coverage will be understandable, influential, vigilant, solution-oriented, and fair-minded. Together we can make a difference.
Keywords: Nigeria, biosecurity, mpox
Topics: Biosecurity
Get alerts about this thread
0 Comments
Oldest

Matt Field
Matt Field is an associate editor at the Bulletin of the Atomic Scientists. Before joining the Bulletin, he covered the White House,... Read More

Dimie Ogoina
Prof. Dimie Ogoina is a Professor of Medicine and Infectious Diseases at the Niger Delta University and an infectious diseases physician at the Niger... Read More