Epic fail: Why the US wasn’t prepared for the coronavirus pandemic
By Daniel M. Gerstein | April 24, 2020
 A shipment of medical equipment from the Strategic National Stockpile arrives in South Carolina. Many states have reported difficulty obtaining the personal protective equipment and other supplies they need to combat the coronavirus outbreak. Credit: South Carolina National Guard.
A shipment of medical equipment from the Strategic National Stockpile arrives in South Carolina. Many states have reported difficulty obtaining the personal protective equipment and other supplies they need to combat the coronavirus outbreak. Credit: South Carolina National Guard.
By the end of February, two months after China reported a mysterious cluster of pneumonia cases to the World Health Organization, the disease we now know as COVID-19 had already claimed almost 3,000 lives. The new coronavirus had spread to 53 countries and sickened some 85,000 people, including more than 60 people in the United States.
But despite the Trump administration implementing a partial travel ban on China on February 2, and travel restrictions on Europe shortly thereafter, the US government was not marshaling a strong response to the crisis. It was not until March 13 when President Donald Trump declared a national emergency that the government’s response became fully engaged. By then, of course, the disease was already spreading throughout the country.
Early on in the outbreak, at a time when better preparations could have been made to forestall the worst impacts of a broad outbreak, the federal response was failing. To paraphrase a former senior emergency management official in Chicago, the cavalry was not coming. Biosurveillance data on the scope of the outbreak wasn’t being heeded. Disease tests and vital medical equipment were not being supplied. The network of officials and offices related to emergency management that had trained together on how to respond to a pandemic had been superseded by an ad hoc White House task force.
Understanding the shortfalls in the federal role to date will be essential in mitigating the effects of, responding to, and recovering from COVID-19, as well as better preparing for future events. There are at least three important areas where the federal government hasn’t played the role it should have.
Inadequate biosurveillance. The roots of why the federal response has been so halting during the first few months of the COVID-19 pandemic can be traced back two decades, to a prior era when US officials were becoming acutely aware of the potential for a major biological incident.
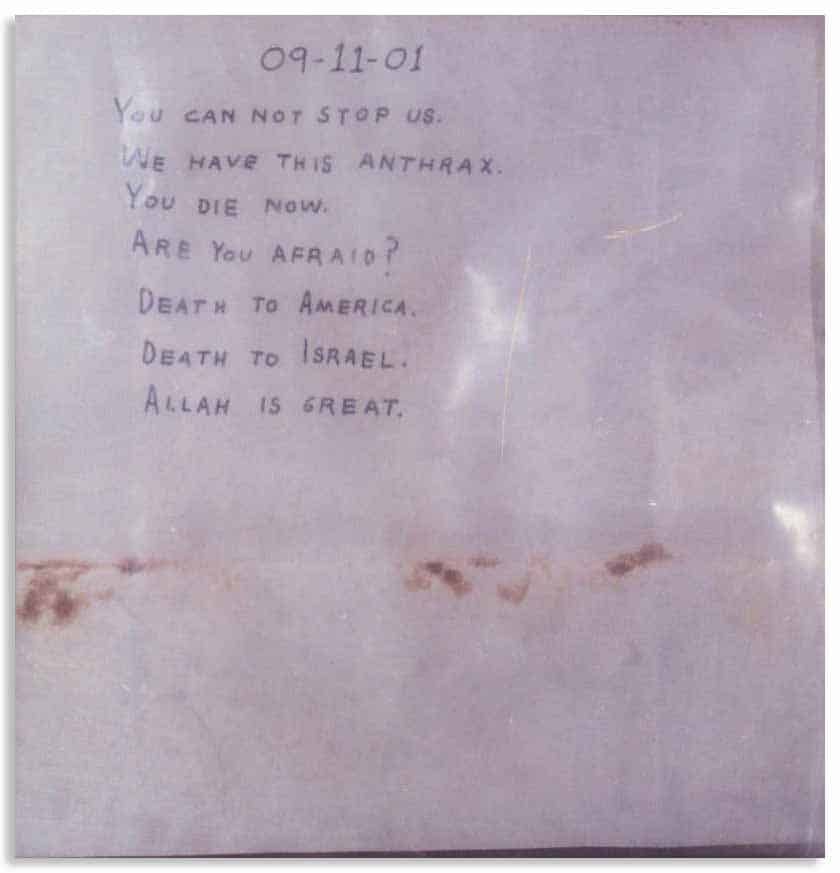
The 9/11 terrorist attacks were the last events to expose a national vulnerability even remotely comparable to the COVID-19 pandemic. Shortly after the attacks, a scientist working at an Army disease research lab added to the unease that had settled on the country by allegedly sending out letters filled with deadly anthrax spores to politicians and media figures. The so-called Amerithrax attacks sickened 17 and killed five, providing a case study for why officials needed to bolster national biodefense.
During the post-9/11 era, officials gave particular attention to improving the country’s capabilities in biosurveillance, defined by the White House as “active data-gathering with appropriate analysis and interpretation of biosphere data that might relate to disease activity and threats to human or animal health.” Government offices undertook myriad activities in the name of biosurveillance. Strategies were written. Training was conducted and exercises were held. Offices like the National Biosurveillance Integration Center were created to integrate “information from thousands of sources about biological threats” to improve “early warning and situational awareness.”
At the end of the day, biosurveillance comes down to having the capacity to sense that a disease is present, so actions can be taken to halt its spread. It comes down to using testing and diagnostics to determine who is and who has been infected, conducting contact tracing to identify who might have been exposed so they can take mitigation protocols, and sharing information, so public health officials can understand how the disease has or has not been controlled. Armed with this biosurveillance data, public health professionals can make data-informed recommendations, and leaders can take action.
In the years following 9/11, biosurveillance systems and plans were put in place to provide the government an opportunity to watch for and react to something like a pandemic virus. But despite strong pronouncements and good intentions, funding shortfalls, organizational disfunction, and problems with information sharing have long confounded federal efforts. By the time COVID-19 first appeared, three different presidential administrations had struggled to develop an effective national biosurveillance system.
All this is not to say that parts of the US government, such as the Centers for Disease Control and Prevention (CDC) and the National Center for Medical Intelligence within the intelligence community, aren’t tasked with biosurveillance responsibilities, but rather that, overall, it’s difficult to argue that the biosurveillance system operates like a well-oiled machine. Both organizations have raised concerns about COVID-19 since early January; however, these admonitions were largely unheeded by the administration until mid-March.
Failures in developing a timely testing protocol for diagnosing the disease contributed to biosurveillance shortfalls and the ineffective national response to COVID-19. The test for the coronavirus developed by the CDC was not accurate and had to be recalled, causing important delays in understanding the spread of the disease in the United States. Even now, the rate of testing lags behind requirements, and there are not enough tests to go around, a major problem for states as they begin to consider lifting stay-at-home orders and easing social distancing restrictions.
A disrupted emergency response network. After 9/11, government officials aggressively developed a so-called national exercise program designed to bring key stakeholders together to force them to confront various scenario-based national emergencies, from hurricanes and tornados to cyberattacks and pandemics. The exercises are intended to test preparedness and response systems as well as support functions and communications chains. The scenario-based exercises are designed to place the actual decisionmakers and specialists throughout the government in difficult and complex positions that require them to react to constantly changing inputs and new information. When the president stood up the coronavirus task force at the end of January and subsequently replaced Secretary of Health and Human Services Alex Azar as its head, officials across the government found themselves dealing with a different system than the one they had trained on.
Ironically, standing up the task force, which was intended to organize the federal fight against COVID-19, disconnected some of the relationships that were important for conducting a coherent emergency response. Many of those relationships ran down from Azar’s office and into state public health offices that were in charge of their states’ responses. Emergency management personnel in state and local offices found it harder to make decisions on how to respond to the crisis. Normal chains for distributing information or supplies didn’t work as well. Unfortunately, not relying on established emergency-management doctrine at the federal level has exacerbated the confusion at the state and local level as well.
By the end of February, Trump replaced Azar and put Vice President Mike Pence at the helm of the coronavirus task force, a role in which Pence has basically been getting high marks as a stabilizing influence. Nonetheless, when the administration or the president shuffles the deck and as officials fall in and out of favor, there can be real-world implications.
Supply chain (mis)management. State governments across the country are finding they are in a competition with other states and the federal government over medical supplies. They’re being left to fend for themselves, and the federal government isn’t taking control of the supply chain to efficiently distribute resources.
The pandemic is highlighting the need to rethink how supplies are stored and distributed in an emergency. In particular, it’s casting a harsh spotlight on the Strategic National Stockpile. Originally created in 1998, the stockpile of emergency supplies and medications is maintained by the assistant secretary for preparedness and response within the Department of Health and Human Services. While the stockpile was designed to provide support during a pandemic response, the level at which it was provisioned and the types of vaccines and therapeutics it contained indicate there was a predisposition to preparing for a bioterrorism event or a much smaller public health emergency, such as the 2014 Ebola response.
General equipment in the stockpile such as personal protective equipment and ventilators would be useful in either a pandemic or bioterrorism event, but the stockpile was not envisioned to have enough for supplying a national crisis of this magnitude. The stockpile just doesn’t have the amounts of the supplies governors say they need to fight COVID-19. That’s a big part of the reason many states have been left to scour the open market. The Trump administration meanwhile, changed its definition of the stockpile’s purpose midway through the pandemic, contextualizing it more as a “stopgap” than a primary resource for states to use.

A make-over for emergency response. Trump’s direction to governors to “step up efforts to get medical supplies” overturned preparedness and response procedures that have evolved since the Congressional Act of 1803, which provided federal assistance to a New Hampshire town following a fire.
Much of the way the United States thought about emergency management before the current pandemic traces directly back to this history. Emergency management in the United States is based on the understanding that all initial response is local. When local authorities no longer have the capacity to mount an effective response, states provide necessary support. When the state capacity is exhausted, the president can make what’s called a Stafford Act declaration and provide federal support for disaster relief.
Two hundred-plus years of thinking and practice in the field of emergency management have produced a system that imagines a strong federal response to disasters. Now, US emergency management experience seems to be getting a make-over. Following months of criticizing the support they’ve been receiving from the federal government, state governments have begun to form pacts to coordinate their response to the outbreak and sometimes even to bypass the federal government.
Despite three successive presidential administrations that placed substantial emphasis on biodefense, the COVID-19 crisis has exposed underlying cracks in the national preparedness and response system. Going forward, the United States will need to question and in some cases relearn the lessons of crisis response and emergency management. Undoubtedly, national funding will need to be reconsidered to ensure that crisis response budgets are aligned with American priorities. Just as in the aftermath of other response failures in US history—Hurricane Katrina and the terrorist attacks of 9/11 come to mind—a public reckoning needs to occur, if the failures of the federal government are to be well-enough understood to reduce the probability that they will recur.
Together, we make the world safer.
The Bulletin elevates expert voices above the noise. But as an independent nonprofit organization, our operations depend on the support of readers like you. Help us continue to deliver quality journalism that holds leaders accountable. Your support of our work at any level is important. In return, we promise our coverage will be understandable, influential, vigilant, solution-oriented, and fair-minded. Together we can make a difference.
Keywords: 9/11, Amerithrax, Coronavirus, anthrax, biosurveillance, emergency management
Topics: Biosecurity

Daniel M. Gerstein
Daniel M. Gerstein formerly served as the acting undersecretary and deputy undersecretary in the Science and Technology Directorate of the Department... Read More













No credible stockpile strategy could begin to match the requirements of a pandemic. Historically the stockpile was backed up by U.S. manufacturing that could surge as the stockpile was depleted. The Obama free trade deals moved most of this manufacturing overseas–thus the U.S. is at the end of the supply chain–adding many months to any effort to rebuild production capability. If one going to fix this problem, have to bring manufacturing back to the U.S.